“Yes, people pull the trigger‑ but guns are the instrument of death. Gun control is necessary,
and delay means more death and horror”
Eliot Spitzer.
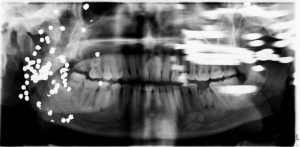
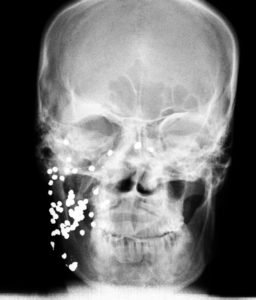
A patient presents with a reduced mouth opening since 12 years. He had a ballistic trauma about 14 years back in the mid-facial region. He had lost his right eye in the procedure of surgery for the same. A few of the extra-oral radiographs are attached here to have a clear picture multiple pellets spread diffusely in the patient’s maxillo-facial region.

Gunshot injuries are on a rise in both developed and developing countries, which is probably due to increased access to firearms. Gunshot injuries cause profound morbidity and significant mortality, especially for the injuries to the neck and maxillofacial region. This is due to the complex anatomy and the presence of various vital structures in this region. The extent of damage is dependent on a number of factors, such as magnitude of energy transferred, distance travelled by the missile, type of bullet and the structures encountered before and on penetration. Foreign objects such as dental instruments, burs, dental materials and a solitary bullet may remain isolated by encapsulating themselves with a granulation tissue reaction, and hence has very little danger. The presence of a foreign body such as a bullet can cause infection and poisoning.
Gunshot injuries continue to fascinate the public, researchers, and clinicians due to the emotional and legal issues it elicits, as well as the extreme morbidity and mortality associated with it. Gunshot injuries, like any other trauma, mainly affect the male gender. In a retrospective study by Odai et al. out of 47 cases, 74.5% of the victims were males under the age group of 20–39 years with peak incidence seen in 20–29 years age group, with almost half of the injuries occurring in daylight. Bullet injuries are divided into high velocity (>2000 ft•s−1) and low velocity (<2000 ft•s−1). A high velocity bullet is likely to lead to quick and
fatal injury to the victim, whereas a low velocity bullet may result in a nonfatal injury. Low velocity firearms mainly include hand guns and shotguns. High velocity firearms, on the other hand, includes missiles or battlefield injuries. Based on the range, gunshot wounds have been classified into three types;
Type I injury (long range of over 7 yards) penetrating subcutaneous tissue and fascia; Type II (range of 3 to 7 yards) penetrating the body cavities;
Type III injury (Blast injury, less than 3 yards).
Extensive soft tissue damage is usually seen in Type II and Type III injuries because, in these injuries, the patients frequently have extensively lacerated and contused wounds with
bony injuries. The degree of bullet fragmentation is also affected by bullet construction. The presence of a full or partial metal jacket has a major effect on deformity. Bullets with full metal jackets often remain in one piece and usually do not deform significantly. These projectiles typically do not leave a trail of lead fragments along their path. On the other hand, semi-jacketed, hollow-point, non-jacketed, and soft-point bullets tend to deform on impact or break apart, leaving a tell-tale trail of metal fragments through the soft tissue. Glezer et al. divided shotgun injuries to three types focusing on the surface area of the pellet scattered.
Type I: Injuries result when scatter is contained within an area of 25 cm2 and the pellets act as individual missiles.
Type II: Injuries were defined as pellet scatter contained within an area of 10–25 cm2.
Type III: Injuries result from scatter contained within an area of less than 10 cm2.
Fragmentation of high velocity bullet creates a lead snowstorm appearance on radiographs. The area over which the lead snowstorm fragments are deposited in the soft tissues widens as the distance from the entry site increases. Thus, a conical distribution of lead fragments is seen on the radiograph with the apex of the cone pointing toward the entry side. The Gussack and Jurkowich system divided the face into entry zones I, II, and III. Zone I was superior to supraorbital rims, zone II was from supraorbital rims to the oral commissure, and zone III was below the oral commissure. The Gant and Epstein system was further modified by Dolin et al. into zones A, B, and C. Zone A represented the lateral face, zygomatic arch, and the mandibular ramus; zone B represented the anterior midface; and zone C represented the anterior mandible. Cole et al. and Chen et al. later simplified this and designated two entry zones, that is, the face and mandible. This is of particular importance, because the maxilla and the mandible show different and distinct patterns of injury. Craniofacial trauma associated with gunshot injury typically involves both functional and aesthetic deformities, leading to mental and social problems. The major complications arising due to bullet injury in head and neck region are presented as below.

Bullet tracts in gunshot victims have been categorized in one of four ways:
• Through and through
• Graze (i.e., tangential without distinct entrance and exit wounds)
• Retained in the body with bullet palpable under the skin
• Retained in the body with bullet not palpable under the skin.
As the projectile enters the victim, the different layers of tissue react according to their specific properties. Injuries to the dermis include abrasion, impaction of particulate matter, and contusion. At close ranges, burning and implantation of powder and residue may occur and may result in a tattoo. After the projectile passes through the skin, it encounters muscle tissue, which is very elastic and may sustain deformation of as much as four times the diameter of the projectile. On a cellular level, the muscle along the pathway of the projectile becomes devitalized and necrotic. As the projectile travels, it may also encounter other surrounding vital structures such as nerves and blood vessels. Vessels may be ruptured, crushed, or sheared, and spasm may occur. These injuries may result in hemorrhage and in the formation of thrombi and hematoma. Sensory and motor nerves may be damaged. When sensory nerves stretch, anesthesia and paraesthesia result; when motor nerves stretch, conduction deficit and loss of function occurs. The minimal projectile velocity required for bone fracture is 65 m/s. Bone is very inelastic; therefore, the type of injury that occurs depends on the type of bone encountered by the projectile. Injury to the cancellous bone usually results in a defect of the drill-hole type. Injury to cortical bone or teeth usually results in shattering. The resulting fragments may act as secondary projectiles and may pose an aspiration risk. In the present case, there was a gradual decrease of mouth opening, probably due to the low velocity gunshot injury causing soft tissue injury to the muscles and the blood vessels leading to spasm. Fernandes and Fernandes reported a case with foreign bodies remaining clinically silent for more than 12 years, and suggested that management of such an asymptomatic patient should include periodic follow-up with measurement of whole blood lead level. The patient must be advised to have a diet rich in vitamin C, calcium and iron because these decrease absorption of lead. If the lead level rises to almost toxic levels, administration of chelating agents with removal of the source of lead is recommended. Ghezta also reported a case with radiographic findings of foreign bodies remaining clinically silent for more than 3 years. Computed tomography (CT) and magnetic resonance imaging (MRI) can be found useful in the evaluation of gunshot wounds. Cone-beam CT (CBCT) scans may be found even more useful as it leads to fewer artefacts. Retained bullets rarely cause problems of delayed infection and late neurological decline, and only if a neurological deficit develops, which is possible after many years, should surgical intervention be considered.
“Gun control isn’t about guns. It’s about us the human beings.” Facial gunshots should be managed as any other type of facial trauma with initial resuscitation and wound care. Significant attention needs to be drawn toward the presence of retained lead bullets in the body. Foreign bodies embedded in tissues do not necessarily result in clinical presentation and remain asymptomatic for a prolonged period of time.