
I investigated………….
It seemed at first a new kind of invisible light.
It was clearly something new
Something unrecorded………..
There is much to do……
Sir Wilhelm Roentgen
A beam of x-ray photons that passes through the dental arches is reduced in intensity (attenuated) by absorption and scattering of photons out of the primary beam. The pattern of the photons that exits the subject, the remnant beam, conveys information about the structure and composition of the absorber. For this information to be useful diagnostically, the remnant beam must be recorded on an image receptor. The image receptor most often used in dental radiography is X-RAY FILM. Dental radiology uses different sizes of films appropriate to be used intraorally or extraorally. It helps us to record the information regarding the object (tissue) through which the X-rays pass. It helps in diagnosis and treatment of different diseases affecting the patient.
Historical background

It is indeterminate who took the first ever dental radiograph, yet the honors are most genuinely shared between the Germans, Koenig and Walkhoff, Frank Harrison in Britain and C. Edmund Kells in New Jersey, every one of whom were creating improvised but identifiable dental ‘skiagrams’ in pre-spring and late-winter of 1896. Dr Friedrich Otto Walkhoff; DDS, MD (1860-1934) a dental practitioner in Brunschweig, Germany, was done with his first dental radiograph within 14 days of the announcement about the Roentgen rays penetrating the solid substances insusceptible to the visible light. He took a conventional photographic glass plate, enclosed it by the rubber dam, place it in his mouth between the teeth and the tongue so he could steady the plate with his tongue, and after that lay on the floor for 25 minutes so that the plate is exposed to x-rays, which was too long a methodology and the way too expensive. The image he acquired was of the crowns of the maxillary and mandibular teeth. It was, in fact, the first bitewing radiograph, proving that “experimenters are the shock troops of science”. Walkhoff proceeded with his experimentation with radiography, and after 2 years, in April 1898, he prevailing with regards to making extraoral images with an exposure time of 3
0 minutes. In 1896, Otto Walkhoff and Fritz Giesel set up the very first dental roentgenologic research laboratory on the planet. Dental radiographs were likewise made by Professor Wilhelm Koenig Wilhelm, PhD of Frankfurt in February 2, 1896. Later Giesen, Germany, made a series of 14 dental radiographs of his own mouth. Requiring just 9 minutes of exposure time for each film, they demonstrated the restorations in some of the teeth. Around the same time, Frank Harrison (England) made a dental radiograph utilizing a 10-minute exposure time. William J Morton (1845-1920), a New York doctor, made the first recorded dental radiograph in the United States in April 1896. The first machine wrapped dental X-ray film packet, called Regular film (Kodak), turned out to
be commercially accessible in 1919. It was a single emulsion, though slow yet delivered sharp images. In the 1920’s cellulose nitrate base was utilized which was highly inflammable and when consumed, discharged huge amounts of toxic gases. In 1924, non-inflammable cellulose triacetate came into picture and was promoted. But, it had a disadvantage of being costly, subject to mold, wrinkled and tended to break.
Meanwhile in the same year, double emulsion films were introduced which had advantage of increased film speed, reduction in exposure by 50% and reduction in the tendency of the film to curl when dried. It was commercially marketed as Radiatized film (Kodak). In 1940, the Ultra speed (Improved Radiatized) films wound up accessible. The ‘D’ speed films were intr
oduced in the 1950. In the 1960s, a film base of polyester (Dacron) was presented and has been the material of choice, with the benefit of being stronger, henceforth thinner films can be made and it doesn’t tend to wrap. The Ekta (E) speed film (Kodak), presented in 1980s has again reduced the exposure by 50 percent.
Ektaspeed plus (E plus) films were launched in 1994 with the same sensitivity as that of the E speed films but with an improved resolution. 2000 was the year for F speed film (in sight) manufactured by Kodak. Reviewing the literature reveals:
1) 30-40% reduction in exposure after switching from D- to E-speed film
2) A reduction of 20-25% in exposure when the films used were switched from E- to F-speed film, and
3) Switching from D- to F-speed film produced a 60% reduction in exposure
How the dental x-ray films are classified??
The X-ray films are classified according to: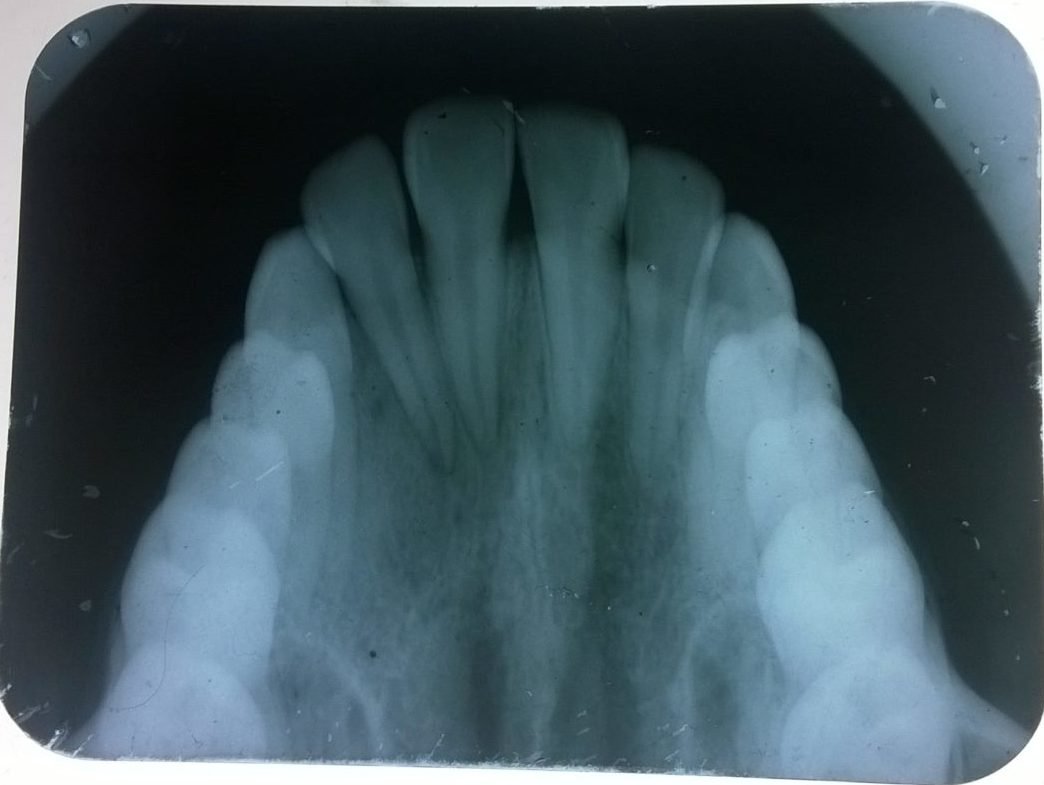
A. Their use
-
- Intraoral films.
- Periapical films
- No 0 for children.
- No 1 for anterior adult projections.
- No 2 for standard adult projections.
- Occlusal films.
- Bite wing films.
- Periapical films
- Extraoral films.
- Intraoral films.
B. The coating of emulsion
-
-
- Single coated: These produce better and sharper images but the exposure to the patient is more, therefore mostly used in Industrial Radiography.
- Double coated: These films have emulsion on both sides. Most dental films are double coated. These allow for less exposure to the patient.
-
C. The speed of the film
-
-
- Slow films: These have a very small grain of silver bromide and emulsion is on one side only. Therefore it gives better definition but the exposure required is more and are thus not routinely used. Their speeds are denoted by A, B, C.
- Fast films: These have a larger grain size and the emulsion is on both sides. Their speeds are D-ultra speed, E- ekta speed and F- ultra ekta speed.
- Hyper speed G: This is a 800-speed film that can half the patient exposure without blurring image quality
-
D. Packaging
-
-
- Single film packet.
- Double film packet: Two films are placed close to each other, when they are radiographed the second film serves as a duplicate.
-
E. Use, non-use of screens
-
-
- Screen films
-
- Sensitive to blue light, e.g. calcium tungstate Screens.
- Sensitive to green light, e.g. Rare Earth Screens.
-
b. Non-screen films.
F. Barrier envelopes
-
-
- With barrier envelopes: these ensure that there is no gross contamination in the dark room.
- Without barrier envelopes.
-
Composition of the x-ray films
Let us discuss about what all a x-ray film composed of in order to get a replica of the tooth and the surrounding structures. Emulsion and base are the two principal components of the x-ray film.
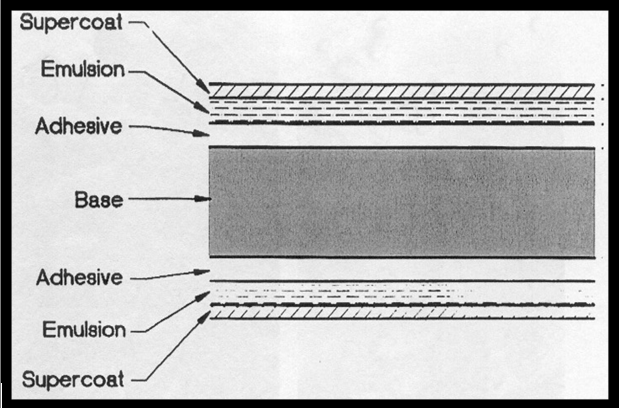 Cross-section of x-ray film
Cross-section of x-ray film
Emulsion
Emulsion consists of silver halide grains and a vehicle matrix. Silver halide grains, chiefly the silver bromide crystals are sensitive to x-radiations and visible light. The increased sensitivity of the ultra speed film is because of the additional larger sized iodide crystals, which disrupts the bromide crystals. InSight films does not use the iodide crystals.
Sulfur containing compounds, when used in trace amounts, increases the photosensitivity of the silver halide crystals. The tabular grains of the InSight film are oriented parallel with the film surface to offer a large cross-sectional area to the x-ray beam. As a result, InSight film requires only about half the exposure of Ultra-Speed film.

All the crystals are suspended in the gelatinous or non-gelatinous vehicle matrix. An adhesive material helps keeping a good contact between the emulsion and the base. An overcoat of an additional layer of vehicle acts as barrier and helps protect the film from damage by scratching, contamination, or pressure from rollers when an automatic processor is used.
Direct exposure films are intended to be directly exposed by x-rays and are used widely in dentistry as intraoral films.
Base: Polyester polyethylene terephthalate is the material used in the base of the film. A 0.18mm thick base supports the emulsion. In order to have an easy handling of the film, base must have the proper degree of flexibility and should be able to withstand the processing solutions. When the cellulose nitrate films are decomposed many harmful gases are released including nitric oxide (NO), nitrogen dioxide (NO2), nitrous oxide (N2O), camphor vapors and tarry residues. Hence, the non-inflammable acetate polyester when used as base material, the films are known as Safe Films.
What is the speed of the Intraoral film??
The speed of the film is the amount of radiation required to produce a radiograph of standard density. Film speed, or sensitivity, is determined by:
-
-
- The size of the halide crystal.
- The thickness of the emulsion.
- The presence of special radiosensitive dyes.
-
Larger the crystal size, faster the film speed, at the cost of the contrast quality of the image on the film. The larger silver halide crystals in the emulsion respond more quickly to the x-radiations and hence, less radiation exposure. The films are given speed ratings from A speed (the slowest) to F speed (the fastest). Only D speed and E-speed are used for intraoral radiography.
As the direct exposure intraoral films are used for varied purposes, they come in various sizes. All the sizes are presented pictorially.

Parts of the intraoral x-ray films
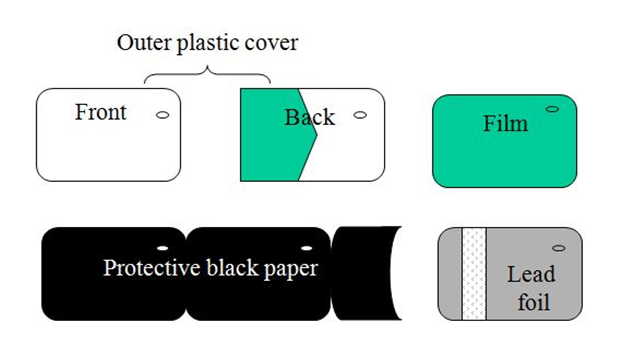 The pictorial representation of each part of the x-ray film from outside to inside shows:
The pictorial representation of each part of the x-ray film from outside to inside shows:
Outer plastic cover: It is made up of soft vinyl and is hermetically sealed which makes the film semi-stiff, moisture proof and light proof. This outer wrapper has two sides, one is the tube side and the other is the label side. The tube of the plastic cover is white in color embedded with an elevated occlusal dot present at one corner. While the intraoral placement of the film, this occlusal dot has to be considered which is always placed towards the incisal/ occlusal surface of the tooth of interest? The corresponding embossed dot helps while mounting the radiograph in order the side of the dental arch exposed. The label side is color coded and has a flap to open the film packet. Color codes are used to distinguish between one film and two film packets, and between speeds of the film.
Beige=F speed, 2 films
Pink=E speed, 2 films
Dark gray=D speed, 2 films
Liliac=F speed, 1 film
Blue=E speed, 1 film
Pale green=D speed, 1 film.
The information printed on the label side of the film are:
-
-
- A circle or dot that corresponds with the raised identification dot on the film
- The statement, “opposite side of the tube”
- The manufacturer’s name.
- The film speed.
- The number of films enclosed.
-
Lead foil: A thin lead foil sheet is placed remote to the tooth under consideration and the X-ray tube. The foil absorbs most of the x-rays and does allow them to pass through and reach the tongue and other oral tissues. It also absorbs the back scatter radiation and thus prevents fogging of the film which would otherwise cause a loss of important diagnostic detail. A secondary function of the lead foil is to give sufficient but not excessive rigidity to the whole film packet. If the film packet is placed reverse in the mouth, the shadow of the foil is seen on the resultant radiograph as tyre track marks or herring bone appearance, which is the embossed pattern placed on the lead foil by the manufacturer.
Black paper: It wraps the film and protects it from any light leak.
X-ray film: It is a translucent film with rounded corners and an embossed raised dot for orientation.
Inference
The intraoral radiography is a boon in the field of dentistry as it helps in diagnosing the odontogenic (tooth-related) lesions along with the surrounding osseous structures. The small sized dental x-ray films representing the 2-dimensional image of the 3-dimensional structures found a great help in the routine dental diagnostics.
Sometimes the smaller things take up the most important information



